
Digital dentistry
Today’s scanners are comparable to a digital camera from the 1990s.
All materials and methods investigated for three-unit bridges resulted in comparable internal fit.
Composite blocks for milling restorations released insignificant amounts of monomers.
“Digital manufacturing using intraoral scanners appears to provide equivalent fit compared to conventional technique for smaller prosthetic constructions. Milled composites have a less toxic potential compared to traditional light cured directly placed composite restorations.”
These conclusions came when NIOM staff (senior scientist John Tibballs, chief engineer Lene Grutle and head of laboratory Hilde M. Kopperud) in collaboration with prosthodontist Bjørn Einar Dahl from University of Oslo discussed digital dentistry at the annual conventions of the Norwegian and the Swedish Dental Associations.
The accuracy of a digital impression depends on both the scanner’s characteristics and the operator’s skills, said Tibballs. The major challenge is the size of the scanner head, and thus the quality of the camera for which there is space. Today’s cameras have a limited number of sensors comparable to a digital camera from the 1990s. As a result the uncertainty in stitching data together can be high, for single crown approximately 80 µm and for a whole tooth arch approximately 400 µm. For a single crown, a good scanning strategy can compensate but for long scans the uncertainty grows markedly.
Tibballs heads the working group within the International Standardization Organization, ISO, which develops test standards for both extra- and intra-oral scanners. With an approved standard, manufacturers who supply intraoral scanners and their customers will be able to judge the indications for which direct digitization is suited. The standard gives the manufacturers a measure of their progress towards a scanner for all intra-oral situations from single post to full jaw prostheses.
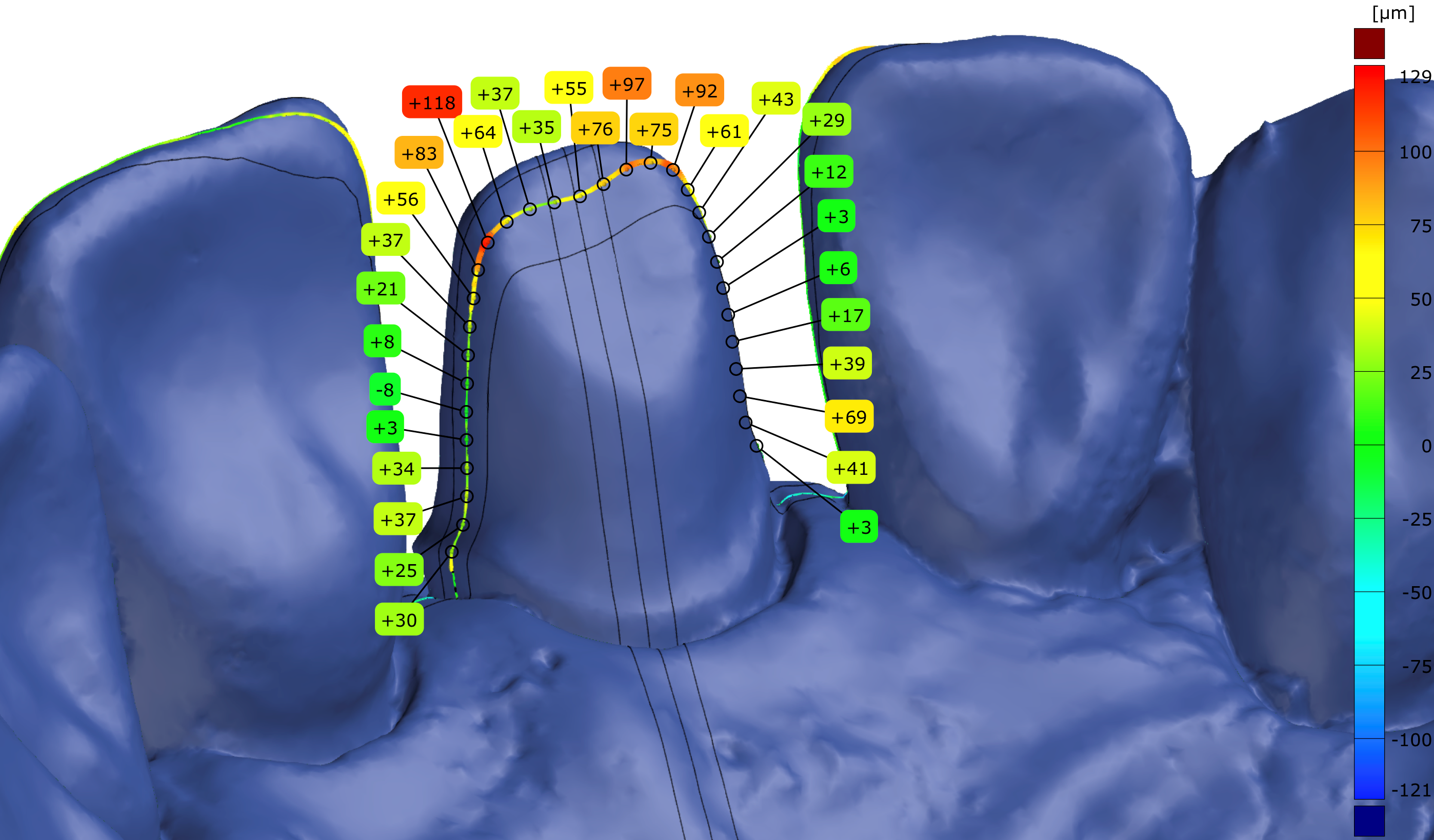
Lines show where digital measurement of the internal fit was made.
Dahl had compared the adaptation, or internal fit, of single crowns and three-unit bridges made from different materials (ceramics and alloys) and digital techniques, to restorations made with conventional lost-wax and metal casting technique. The internal fit was determined by two different digital measuring methods; dual scan and triple scan. Both methods are relatively new and it was important to evaluate them. Single crowns made with conventional technique had the narrowest cement space compared to digitally produced crowns. For all crowns the cement space was within what is termed clinically acceptable. The statistically significant difference in cement space was not observed for the three-unit bridges. The cement space on the “external”, or most distal, surfaces of the bridge was larger than the cement space of the “internal”, or most mesial, surfaces. It is unknown if this is of clinical importance. As for the evaluation of the measuring methods it was concluded that both methods seemed to be appropriate for the investigation of internal fit.
Milling blocks with test specimen.
Grutle and Kopperud stated that if milling of composite restorations is to be an alternative to directly placed composite restorations, they should have a higher degree of cure and a lower release of monomers. Five different milling composites were examined at NIOM and the release of monomers was evaluated. A highly sensitive analytical instrument, UPLC/MS-MS, enabled the detection and quantification of very small amounts of monomers in the elution medium (75 % ethanol). In comparison, the values were in the order of 1/1000 of the release of monomers from directly placed composite restorations.
